Carpal Tunnel Syndrome:
Clinical Features, Diagnosis, and Management
Lancet Neurology
November 2016; Vol. 15; No 12; pp. 1273-1284
Luca Padua, Daniele Coraci, Carmen Erra, Costanza Pazzaglia, Ilaria Paolasso, Claudia Loreti, Pietro Caliandro, Lisa Hobson-Webb. This study cites 113 references.
KEY POINTS FROM THIS ARTICLE:
1) “Entrapment neuropathies are the most frequent mononeuropathies encountered in clinical practice.”
- “In these neuropathies, the nerve is damaged at sites where it passes through narrow, restricted spaces.”
- “Although entrapment neuropathies affect only a small portion of the nerve, they can have substantial physical, psychological, and economic (eg, loss of earnings) consequences.”
2) “Carpal tunnel syndrome [CTS] is the most common peripheral nerve entrapment syndrome worldwide.”
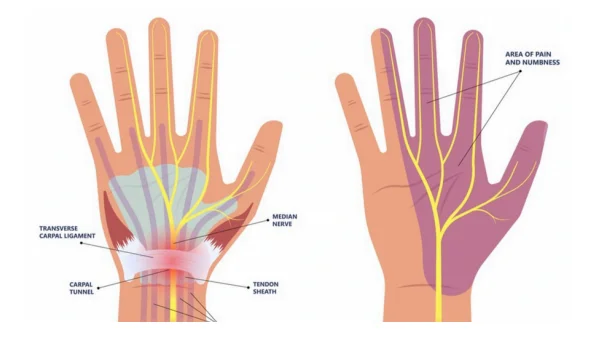
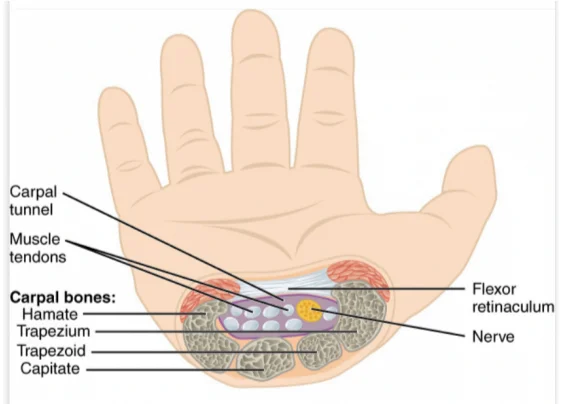
- “It is caused by compression of the median nerve at the wrist as it passes through a space-limited osteo-fibrous canal.”
- “This canal, known as the carpal tunnel, contains the wrist bones, transverse carpal ligament, median nerve, and digital flexor tendons.”
3) “Clinically, one in ten people develop carpal tunnel syndrome at some point.”
4) The prevalence of carpal tunnel syndrome is similar in men and women.
- The highest prevalence is in women aged 65–74 years.
5) “There is a paucity of evidence about the best approaches for assessment of carpal tunnel syndrome and to guide treatment decisions.”
6) “Oedema, tendon inflammation, hormonal changes, and manual activity can contribute to increased nerve compression and sometimes cause pain, as in the case of tendon inflammation.”
- “In more severe cases, weakness of median nerve innervated muscles can occur, resulting in hand weakness.”
7) Risk factors of carpal tunnel syndrome include diabetes mellitus, menopause, hypothyroidism, obesity, arthritis, and pregnancy.
8) “The syndrome is characterised first by intermittent, nocturnal paraesthesias and dysaesthesias that increase in frequency and occur during waking hours.”
- “[Later], loss of sensation develops along with weakness and thenar muscle atrophy later in the disease course, which result from extensive axonal degeneration.”
- Symptoms in the hand “can spread proximally to the forearm, upper arm, and sometimes shoulder.”
- “When patients with carpal tunnel syndrome are asked specifically where their pain and sensory symptoms are, they usually report that the proximal symptoms are characterised by pain and not by numbness, tingling, or other sensory abnormalities.”
- “Assessment of sensory function is not useful unless performed carefully with specific tools (eg, monofilament or static two-point discrimination).”
- Pain is a common symptom in patients presenting with carpal tunnel syndrome in clinical practice, but is not always present; in one study pain was present in only 52% of cases.
9) Popular diagnostic tests for carpal tunnel syndrome include:
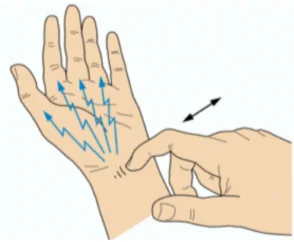
- Tinel’s sign is positive when symptoms are evoked by percussion of the median nerve at the wrist:
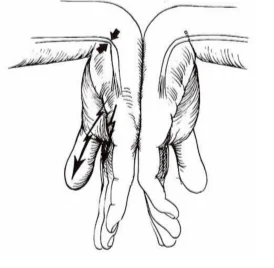
- Phalen’s test is positive with forced compressive wrist posture for 1 min:
10) “Controversies exist regarding the need for confirmatory testing and the role of nerve conduction studies, electromyography, and nerve ultrasonography in treatment decision making.”
- Practice guidelines consider needle electromyography to be better suited to exclude cervical radiculopathy.
- “When clinical signs are present, but no electro physiological abnormalities, then the disease is functionally mild, although there might be severe symptoms.”
11) Ultrasonography is capable of reproducing nerves (fascicles, epineurium, and surrounding structures.
- “Morphological changes of the median nerve are expected in carpal tunnel syndrome, as the compression of the surrounding nonrigid structures alters its shape.”
- “This effect results in a reduction of nerve volume at the site of compression and increased size proximal to the compression.”
- “Ultrasonography can show an increased cross-sectional area of the nerve just before it is flattened at the site of compression.”
12) “An emerging technique for nerve imaging is now available: MRI tractography.”
- “This technique can provide details on morphological damage and inflammation.”
- “Although providing excellent imaging capabilities, use of the technique is limited by cost.”
13) “Cervical radiculopathy is the primary disorder that might be confused with carpal tunnel syndrome.”
- “Cervical radiculopathy is usually characterised by pain in the neck with radiation (often with positive sensory symptoms [eg, paraesthesia or dysaesthesia], sometimes exacerbated by rotation, flexion, or extension of the head) to the upper limb often with typical dermatomal distribution.”
- “Reduced or abolished deep tendon reflexes are typical of radiculopathy.”
- “Needle electromyography and cervical spine imaging can also be useful in differentiating cervical radiculopathy from carpal tunnel syndrome.”
14) Laser therapy
- “Low-level or low-power laser therapy, which exposes tissue to low levels of red and near-infrared light…. is one of the non-surgical options for treatment of carpal tunnel syndrome.”
- “Laser therapy is able to improve function, symptoms, and electrophysiological measures in the short term; results of a randomised controlled study showed that laser treatment is more effective than placebo, especially if it is used in patients with mild to moderate disease.”
- Laser therapy is more effective than placebo, even at 3 months.
15) Therapeutic ultrasound:
- “Therapeutic ultrasound is a treatment approach based on the hypothesis that mechanical waves interacting with the tissues of the carpal tunnel (including the median nerve) will reduce inflammation.”
- Ultrasound therapy is “more effective than paraffin therapy, a deep heat treatment that ameliorates local blood flow.”
16) “Musculoskeletal manipulation is widely used.”
- “This approach includes massage, exercise, and mobilisation of the wrist joint.”
17) An important non-surgical approach is the use of splints.
- They are designed to reduce the mechanical stress due to the contact between the median nerve and the surrounding tissues of the carpal tunnel.
- Splinting and gliding exercises may reduce edema.
18) “Surgical treatment, consisting of release of carpal tunnel content by transection of the transverse carpal ligament, is considered the most effective treatment to alter the relation between content (the median nerve and tendons) and container (the carpal tunnel).”
- “Surgical complications of carpal tunnel release are reported to occur in 1–25% of patients.”
- “One potential severe complication of carpal tunnel operations is complex regional pain syndrome, which presents as hand pain, increased sweating, and vasomotor instability.”
- “Its incidence after carpal tunnel release varies from 2.1% to 5%.”
- “Other complications of carpal tunnel release are scar tenderness, pillar pain (tenderness close to the ligament release), transient neuropraxia, and reoperation.”
- Recurrent symptoms began from 3 months to 4 years after surgery and the mean time between first and revision surgery was 31 months.
19) “Regarding management of carpal tunnel syndrome, both surgical and non-surgical interventions can be beneficial.”
20) “In view of the treatment differences and the potential for surgical adverse events, initial non-surgical management is supported by evidence, with surgical release then being considered for patients with severe or persistent symptoms.” [Important]
21) “Validated patient-centred measures (eg, the Boston Carpal Tunnel Syndrome Questionnaire [BCTQ]) are able to quantify symptoms and disability.”
22) “Patient-centred measures (eg, BCTQ) are crucial for quantifying symptoms and disability, whereas the functional (electrodiagnostic) and morphological (ultrasound) measures are essential for assessing nerve involvement and progression.”
We have reviewed these articles pertaining to carpal tunnel syndrome:
49-06: Peripheral Nerve Entrapment Caused by Motor Vehicle Crashes
07-07: The Double Crush in Nerve-Entrapment Syndromes